I wrote this essay after attending a discussion about health inequalities in Scotland. It isn’t directly about Realistic Medicine, but it sets the background.
INTRODUCTION:
17% of Scotland’s people live in remote and rural areas, nearly a million people, double the population of Edinburgh. (1, 2). They live in one of the most beautiful places on the planet, with one of the lowest population densities in Europe. All of them have a right to be registered with a GP and have access to healthcare that is safe, effective, person-centred, equitable, timely and efficient, as outlined in the Chief Medical Officer’s annual reports. (3)
However, the current challenges facing remote and rural health care teams are barriers to meeting these aspirations. Existing good practice seems to be undervalued, and the principles of the new Scottish GP contract do not seem appropriate for very small and remote clinical teams.
CONTEXT AND BACKGROUND:
We have a shortage of GPs in Scotland, with many areas reporting longstanding and significant levels of vacancies. With shrinking clinical teams, it becomes harder to deliver the additional extras, the enhanced services that were a feature of the previous GP contract; enhanced service contracts became the mechanism for encouraging GP practices to take on additional work for additional income. Increasingly, GPs across the UK have been concerned about secondary care work being shifted out into primary care without adequate funding or support.
In response, the new Scottish GP contract has pared back the requirement for GPs to undertake non-core services, so that they can focus on the core work of providing primary medical services. At the same time, some of the clinical work currently done by GPs could be done by others, such as physiotherapists, pharmacists, psychiatric nurses and others, and the new contract asks health boards to change to this model.
In our rural practices, with small numbers of patients scattered over wide areas, GP practices have been the only realistic option for providing health care services without travelling huge distances. Small teams based round one or two GPs have provided a very wide range of services, taking on additional roles to provide a holistic service. Recruitment, retention, and support appropriate to the area would sustain services.
The rural GPs that I know are proud of the excellent services they can provide to their communities. Being a member of such a community means that rural GPs identify very highly with their patients, their difficulties and aspirations. They are advocates for local health services, with a deep knowledge and understanding of the local population. There is a strong culture of stewardship, of using the resources of the NHS wisely and appropriately for the best outcomes. Rural General Practice has been delivering Realistic Medicine for many years before it was branded and marketed by the Chief Medical Officer for Scotland.
Published data shows that Scotland’s rural areas have a static and unacceptably high level of fuel poverty, (4) with nearly two fifths of residents needing to spend more than 10% of their income to heat one room of their homes to safe levels. Fuel poverty is associated with worse health outcomes.
Populations are older too. In the Western Isles, for example, a quarter of the population is over 65, retired, less economically active, and this number is set to rise to over a third in the next fifteen to twenty years. Older populations have higher rates of multi-morbidity, cancer, falls and frailty, with complex health and social care needs.
Within the last year, the new contract for primary care in Scotland has been voted on and implemented. It has been a radical revision of the way that medical services are provide out with hospitals, aiming to address the shortfall of GPs by increasing access to other healthcare professionals in the context of multidisciplinary teams.
It has come with a new allocation formula, claiming to improve funding for teams providing care for older patients, and improving funding to practices where GP income is low.
THE NEW CONTRACT – DOES IT ADDRESS HEALTH INEQUALITY AND GP RETENTION AND RECRUITMENT?
The new contract has left many rural GPs feeling devalued and disheartened. Their professional raison d’etre has been to provide a holistic service, going the extra distance to ensure that care can be delivered by clinicians who know their patients well, delivered by teams that are stable and supportive.
By breaking these teams up, telling GPs that their enhanced services are no longer required, whilst parachuting in a number of peripatetic staff each working one session a week in each of multiple practices, this all feels like a betrayal. The contract does not value the extended services that make rural practice so effective in delivering rural Realistic Medicine.
While no practice in Scotland will receive less money initially, the Scottish Allocation Formula makes it clear that some practices are more deserving than others. In rural practices and in ‘deep end’ practices, there is little in the way of hope of an uplift. The formula does not recognise adequately the additional costs of running a rural service, the cost of addressing the health needs of rural poverty, of fuel poverty, the personal health and financial cost of travel to care, or the additional costs of professional training and networking.
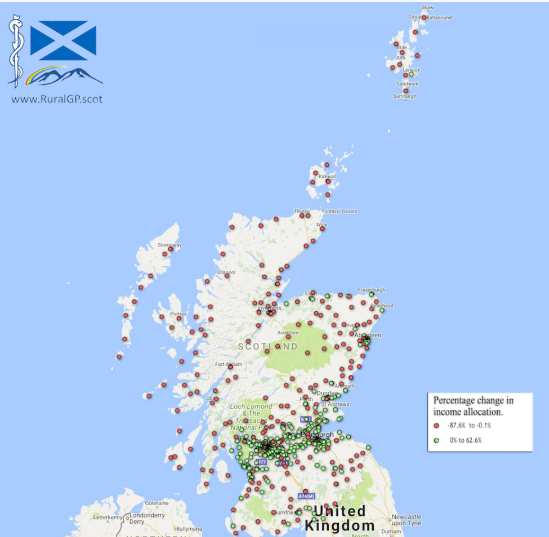
The striking map below illustrates where practices are getting an uplift in funding in green dots. It was put together by Dr G Wheeler, North Uist Medical Practice, from data from the Scottish Government. (5)
At the same time, the impact of other policies is still being felt. Scotland’s broadband and mobile phone networks were designed to reach the majority, rather than the populations that needed them most. Even though broadband roll-out has been trumpeted widely, on the ground in rural areas, the infrastructure is incomplete. Rural practices still don’t have access to new data-collection systems, and wifi is still limiting participation from remote areas.
The new contract does not address rural health inequality and may be contributing to reduced retention. The allocation formula does not address the additional costs of providing health care in rural areas, the need to provide care to small and isolated populations all day every day, the need to provide realistic care in the case of widespread multimorbidity. If a multidisciplinary team is led by a GP now, expanding the team by adding fractions of WTE staff to many practices, makes co-ordinating that team more complex, without solving the recruitment needs.
The new contract in rural areas might mean many more clinical staff each offering only a tenth of a whole time equivalent each, never meeting to form a team. Accommodation for small rural teams doesn’t include space for expanded teams, and there seems to be no plan to address this.
The new contract does not seem to address deep-end health inequality either; their patients suffer from multimorbidity at an earlier age, before funding catches up. Their barriers to engagement and access may be societal rather than geographical, but poverty in both settings makes it harder to overcome those barriers.
The new contract cannot be accommodated easily in rural practice, and many practices feel they stand to lose much of the work that they held in highest value, the ability to go further to address clinical need and provide patient centred care in patients’ own homes and communities.
CONCLUSION
Addressing health inequalities in Remote and Rural, and in Deep-end practices should not be an afterthought. Bolting on solutions after the fact doesn’t seem secure. Is Rural Health Care really an additional extra?
Health policy should address the needs of the most vulnerable people in our country. Addressing the challenges first means that provision is fit for all, not just for the central belt. This ‘Rural First, Deep-end first’ approach is appropriate in many ways, from consultation, to creating policy and developing infrastructure.
Consultation for hard-to-reach areas needs to be more enquiring, more inclusive, more investigative. Relying on representatives means that only the views of a politically minded few are heard. Most GPs are in the service to provide health care, and as our ranks are depleted, fewer and fewer find time to get engaged in political lobbying and research.
Scotland sets itself out as a country where the Government listens to GPs, a country where it is the best place in Britain to be a GP. For those GPs who are working in the poorest, most deprived, most rural, most remote areas, these aspirations are not yet being met. Whatever we set out for the people of Scotland, it should work as well for the people of Barra, as for Barrhead and Bearsden.
REFERENCES:
- http://www.gov.scot/Publications/2018/03/6040/5 (accessed 06.06.2018)
- http://www.gov.scot/Publications/2011/09/29133747/2 (accessed 06.06.2018)
- http://www.gov.scot/Publications/2018/04/4249/0 (accessed 06.06.2018)
- https://www.eas.org.uk/en/fuel-poverty-overview_50439/ (accessed 14.10.2018)
- http://ruralgp.com/2017/12/mapping-out-the-proposed-scottish-gpcontract-allocation-formula/ (Accessed 15/10/2018)